
Glaucoma is a disease that damages your eye’s optic nerve. It usually happens when fluid builds up in the front part of your eye. That extra fluid increases the pressure in your eye, damaging the optic nerve. Glaucoma is a leading cause of blindness for people over 60 years old. But blindness from glaucoma can often be prevented with early treatment.
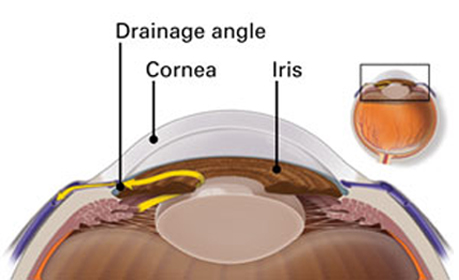
In a healthy eye, excess fluid leaves the eye through the drainage angle, keeping pressure stable.
There are two major types of Glaucoma.
This is the most common type of glaucoma. It happens gradually; where the eye does not drain fluid as well as it should (like a clogged drain). As a result, eye pressure builds and starts to damage the optic nerve. This type of glaucoma is painless and causes no vision changes at first.
Some people can have optic nerves that are sensitive to normal eye pressure. This means their risk of getting glaucoma is higher than normal. Regular eye exams are important to find early signs of damage to their optic nerve.
This type happens when someone’s iris is very close to the drainage angle in their eye. The iris can end up blocking the drainage angle. You can think of it like a piece of paper sliding over a sink drain. When the drainage angle gets completely blocked, eye pressure rises very quickly. This is called an acute attack. It is a true eye emergency, and you should call your ophthalmologist right away or you might go blind.
Here are the signs of an acute angle-closure glaucoma attack:
Many people with angle-closure glaucoma develop it slowly. This is called chronic angle-closure glaucoma. There are no symptoms at first, so they don’t know they have it until the damage is severe or they have an attack.
Angle-closure glaucoma can cause blindness if not treated right away.
With open-angle glaucoma, there are no warning signs or obvious symptoms in the early stages. As the disease progresses, blind spots develop in your peripheral (side) vision.
Most people with open-angle glaucoma do not notice any change in their vision until the damage is quite severe. This is why glaucoma is called the “silent thief of sight.” Having regular eye exams can help your ophthalmologist find this disease before you lose vision. Your ophthalmologist can tell you how often you should be examined.
People at risk for angle-closure glaucoma usually show no symptoms before an attack. Some early symptoms of an attack may include blurred vision, halos, mild headaches or eye pain. People with these symptoms should be checked by their ophthalmologist as soon as possible. An attack of angle-closure glaucoma includes the following:
People with "normal-tension glaucoma" have eye pressure that is within normal ranges but shows signs of glaucoma, such as blind spots in their field of vision and optic nerve damage.
Some people have no signs of damage but have higher than normal eye pressure (called ocular hypertension). These patients are considered "glaucoma suspects" and have a higher risk of eventually developing glaucoma. Some people are considered glaucoma suspects even if their eye pressure is normal. For instance, their ophthalmologists may notice something different about their optic nerve. Anyone who is considered a glaucoma suspect should be carefully monitored by their ophthalmologist. An ophthalmologist can check for any changes over time and begin treatment if needed.
Your eye constantly makes aqueous humor. As new aqueous flows into your eye, the same amount should drain out. The fluid drains out through an area called the drainage angle. This process keeps pressure in the eye (called intraocular pressure or IOP) stable. But if the drainage angle is not working properly, fluid builds up. The pressure inside the eye rises, damaging the optic nerve.
The optic nerve is made of more than a million tiny nerve fibers. It is like an electric cable made up of many small wires. As these nerve fibers die, you will develop blind spots in your vision. You may not notice these blind spots until most of your optic nerve fibers have died. If all of the fibers die, you will become blind.
Some people have a higher than normal risk of getting glaucoma. This includes people who:
Talk with an ophthalmologist about your risk of getting glaucoma. People with more than one of these risk factors have an even higher risk of glaucoma.
The only sure way to diagnose glaucoma is with a complete eye exam. A glaucoma screening that only checks eye pressure is not enough to find glaucoma.
During a glaucoma exam, your ophthalmologist will:
Glaucoma damage is permanent—it cannot be reversed. But medicine and surgery help to stop further damage. To treat glaucoma, your ophthalmologist may use one or more of the following treatments.
Medication
Glaucoma is usually controlled with eye drop medicine. Used every day, these eye drops lower eye pressure. Some do this by reducing the amount of aqueous fluid the eye makes. Others reduce pressure by helping fluid flow better through the drainage angle.
Glaucoma medications can help you keep your vision, but they may also produce side effects. Some eye drops may cause:
All medications can have side effects. Some drugs can cause problems when taken with other medications. It is important to give your doctor a list of every medicine you take regularly. Be sure to talk with your ophthalmologist if you think you may have side effects from glaucoma medicine.
Never change or stop taking your glaucoma medications without talking to your ophthalmologist. If you are about to run out of your medication, ask your ophthalmologist if you should have your prescription refilled.
In trabeculectomy, a flap is first created in the sclera (the white part of the eye). Then a small opening is made into the eye to release fluid from the eye. There are two main types of laser surgery to treat glaucoma. They help aqueous drain from the eye. These procedures are usually done in the ophthalmologist’s office or an outpatient surgery center.
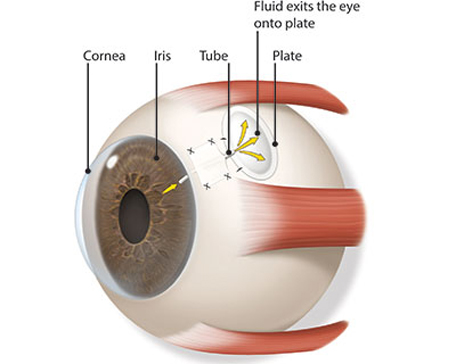
Some glaucoma surgery is done in an operating room. It creates a new drainage channel for the aqueous humor to leave the eye.
Treating glaucoma successfully is a team effort between you and your doctor. Your ophthalmologist will prescribe your glaucoma treatment. It is up to you to follow your doctor’s instructions and use your eye drops.
Once you are taking medications for glaucoma, your ophthalmologist will want to see you regularly. You can expect to visit your ophthalmologist about every 3–6 months. However, this can vary depending on your treatment needs.
If you have any questions about your eyes or your treatment, talk to your ophthalmologist.